
Embryo Banking can be used to postpone having children while pursuing your educational and professional goals.
Impact of Female Age: Female fertility begins to decline many years prior to menopause, despite continued regular ovulations. The likelihood of a successful pregnancy decreases by approximately 10% to 15% each year after the age of 32 and at an even faster rate after the age of 37. Most women aged 42 and older will require Donor Egg In Vitro Fertilization to have a child.
The successful outcome of the Embryo Banking treatment depends primarily on the patient’s age at the time of embryo cryopreservation. Unfortunately, the success rates of Embryo Banking appear to decline significantly for older women (40 years or older).
Treatment Logistics:
Embryo Banking consists of retrieving eggs from your ovaries, fertilizing them with your partner’s semen, cryopreserving the resulting embryos, and storing them for your future use.
Cryopreserved embryos are kept in liquid nitrogen, which allows them to remain in a suspended state, “frozen in time.” The uterus does not “grow old,” so the probability of a successful outcome from cryopreserved embryos is independent of the patient’s age at the time the embryos are thawed and transferred into the uterus.
The probability of conception from frozen-thawed embryos would be expected to be the same as with In Vitro Fertilization when “fresh” embryos are transferred. No increase in chromosomal abnormalities, birth defects, or developmental deficits has been noted in children born from cryopreserved embryos.
Most patients will be able to continue their everyday lifestyles during their treatment.
Embryo Banking is a two-stage treatment. The first phase consists of the development and cryopreservation of embryos:
- Ovarian Stimulation
- Egg Retrieval Procedure
- Fertilization of eggs
- Culture of embryos
- Cryopreservation of embryos
- Embryo storage
The second stage consists of the subsequent Frozen Embryo Transfer cycle.
Ovarian Stimulation: There are several different forms of ovarian stimulation protocols, each with many modifications. Your treatment is always individualized to maximize the probability of a successful outcome.
The selection of an optimal protocol is based on your reproductive history and your pre-treatment evaluation. Below is an example of an Embryo Banking treatment protocol. Your individualized protocol may take less or more time to complete.
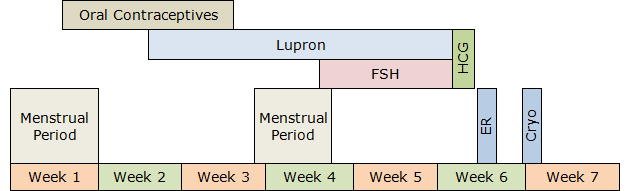
Follicle-stimulating hormone (FSH) or a combination of FSH/luteinizing hormone (LH) hormones will stimulate the production of multiple eggs in the ovaries. They are given once a day or once every other day subcutaneously with tiny needles for approximately ten days.
During this time, your progress is monitored by estradiol (estrogen, E2) and progesterone blood levels and ultrasound examinations.
Ovarian stimulation should result in the development of several eggs in each ovary. The ultrasound image below shows a stimulated ovary. Each of the several follicles (dark circles) contains a microscopic egg.

Egg Retrieval Procedure: The egg retrieval procedure only takes a few minutes.
Under ultrasound guidance, the tip of a thin needle is passed through the top of the vagina into the cul-de-sac (space behind the uterus). The ovaries are located near the bottom of the cul-de-sac, allowing the tip of the aspirating needle to enter the ovarian follicles and aspirate the follicular fluid from them. The fluid is examined under a microscope to identify the eggs.
Fertilization of Eggs: On average, twelve to sixteen eggs are aspirated during the egg retrieval procedure. The eggs are identified under the microscope and placed in petri dishes filled with culture medium. The composition of the medium resembles the fluid secreted by the Fallopian tubes. This allows the eggs and embryos (fertilized eggs) to develop at the same rate as inside the Fallopian tubes.
The male partner collects a semen specimen by masturbation on the day of egg retrieval. The highest quality sperm are extracted from the semen and combined with the eggs three hours after the egg retrieval. This process of in vitro fertilization takes place over several hours during the evening after egg retrieval.
If the male partner has never caused pregnancy, or if your test results indicate a possibility of significant male infertility, Intracytoplasmic Sperm Injection (ICSI) is performed. In ICSI, a single sperm is inserted into an egg. This can significantly increase the probability of normal fertilization for selected patients.
Culture of Embryos: Evidence of fertilization can be seen the next day, 16 hours after insemination. The fertilized eggs are transferred into a growth medium and continue to be cultured.
A normally fertilized egg (zygote) will show two pronuclei representing the genetic material from the egg and sperm.
The following day, embryos should divide into 4 cells and, the day after, into 8 cells.
This picture shows a morphologically exquisite, day three, 8-cell embryo. At this stage, human embryos are still microscopic and invisible to the naked eye.

By the fifth to seventh day after insemination, embryos should reach the blastocyst stage (80 or more cells).
This picture shows an advanced stage of blastocyst development. Notice the central fluid-filled cavity. The cells within the blastocyst have already differentiated into the inner cell mass (at seven o’clock) that will give rise to the fetus and the trophectoderm cells that will form the future placenta.

Cryopreservation of Embryos: Embryos that develop normally are cryopreserved (vitrified). Preparation for the freezing process involves removing water from within the embryos and replacing it with a cryoprotective substance to prevent ice crystal formation during vitrification and subsequent thawing. The embryos are then flash-cooled to −196 °C (−321 °F). Such rapid freezing (vitrification) prevents damaging water crystal formation.
Embryo Storage: Following the cryopreservation process, the embryos are transferred to a liquid nitrogen storage chamber. Theoretically, there is no limit on the length of storage, but conceiving past the age of 40 may result in a high-risk pregnancy.
When you decide to conceive with your cryopreserved embryos, you will have one or two embryos thawed and transferred into your uterus. A large majority of the embryos will survive the cryopreservation and thawing process. The implantation rate of the thawed embryos should be the same as the “fresh” embryo implantation rate.
If you are successful, your pregnancy becomes indistinguishable from conception through intercourse, and your obstetrical care should be no different than if you conceived without any treatment.